Through a coordinated research project, the IAEA has optimized the use and application of the carbon-13 sucrose breath test for assessing nutrient absorption in children. This in turn increases understandings of environmental enteric dysfunction – a disease implicated in stunting, which is a measure of chronic malnutrition.
Even though public health interventions have endeavoured to tackle stunting through food supplementation and improved water and sanitation, children in low- and middle-income countries remain short for their age – a condition that impacts their development and increases their risk of chronic diseases later in life. The most recent United Nations report on global food security and nutrition notably shows that 148.1 million children under five were stunted in 2022. By 2030, stunting is expected to decline by only 3 percent – from 22.3 percent to 19.5 percent, short of the desired target.
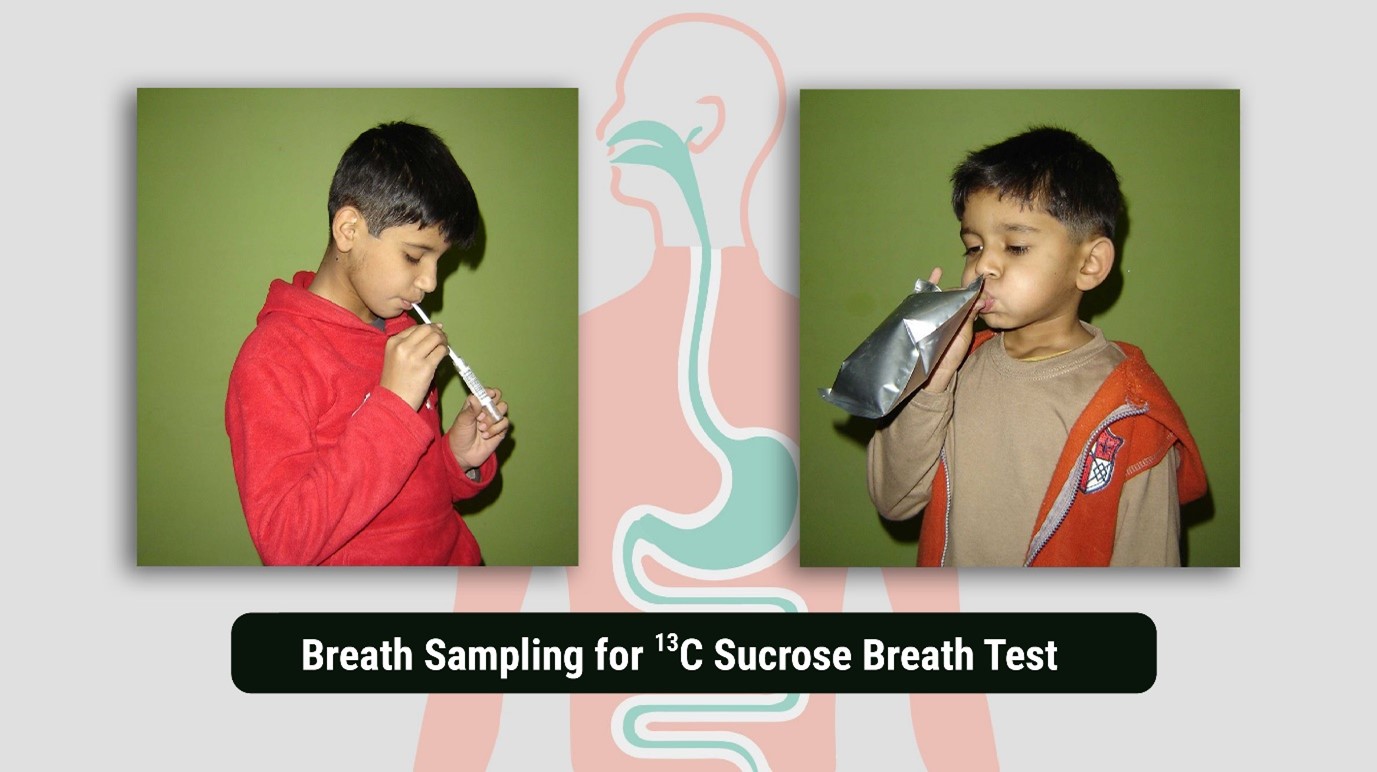
Given its role in poor nutrient absorption, environmental enteric dysfunction (EED) is a significant contributor to the global challenge of stunting in children. EED is an acquired disease of the small intestine characterized by chronic inflammation, poor nutrient absorption, and damage to the small intestine which results in increased “leakiness” and the potential for the uncontrolled movement of pathogens into the body. The disease is thought to be highly prevalent in unsanitary conditions. For children worldwide, particularly those living in such settings, the carbon-13 sucrose breath test serves as a novel, non-invasive tool that can help to assess nutrient malabsorption, which is one of the ways this disease affects children.
Understanding and diagnosing this dysfunction is therefore crucial in addressing malnutrition and improving health outcomes in vulnerable populations.
